Move beyond simple symptom management. This month, we analyse the specific biomechanical anomalies, including the Pivot Point and leg length differences that drive Plantarfasciois and the development of calcaneal spurs.
Clinical Symptoms and Presentation
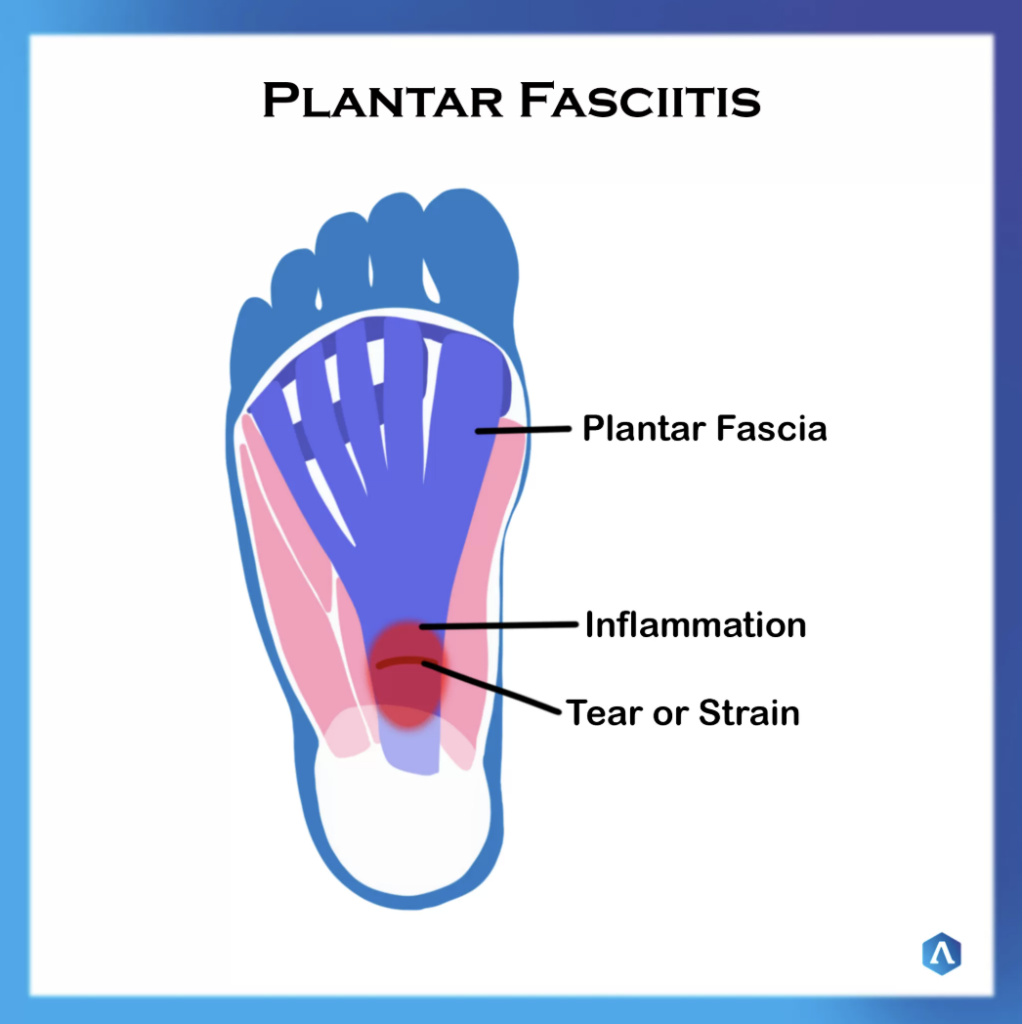
Plantar Fasciitis is a common condition affecting thousands of people daily, characterised by the band of tissue connecting the heel to the front of the foot, seizing up or contracting. Patients frequently describe the sensation as a “hot iron” going through the heel bone. Clinical indicators include:
- Severe to moderate pain upon rising in the morning, often resulting in an inability to walk for 5–10 minutes.
- Difficulty walking after sitting for a period.
- Burning and sharp pain after standing all day.
Biomechanical Causes and Anomalies
The plantar fascia is a major aponeurosis attached at the heel bone (calcaneus) and the metatarsal heads. While injuries can occur during sports or due to tight calf muscles and high arches, excessive pronation is a primary cause, leading to an elongation of the fascia that tears from the heel attachment.
Specific pain locations correspond to distinct biomechanical anomalies:
- Lateral heel pain of the heel due to supination.
- Centre heel pain due to supination, then pronation (Pivot Point).
- Medial heel pain due to excessive subtalar joint pronation.
If only one foot has plantar fasciitis, then this could also be related to leg length difference, where the longer leg rolls in to pronate the foot to level with the shorter leg.
Progression to Plantarfasciois and Heel Spurs
If untreated, the condition may progress to Plantarfasciois, where the body forms adhesions, thickening, and scarring at the attachment site. This is a degenerative state associated with tearing rather than active inflammation. As a compensation for this degeneration, a bone growth known as an Inferior Calcaneal Spur (Heel Spur) may form.


Multimodal Treatment Pathways
A thorough biomechanical assessment is required to determine the actual cause and specific pain points, enabling a tailored treatment plan. Sanctioned modalities include:
- Orthotics: There are many types on the market. The ‘Aspirin’ level from the retail shops, ‘Codene’ level like Crown Medical orthotics (CMO), which are widely used by practitioners and the ‘Morphine’ level, which are made from a cast impression or scan of the foot and are full customised and are very expensive and have no room for error. Medically prescribed innersoles such as CMO or casted orthotics are designed to support, control and align the foot whilst correcting mechanical issues from the feet up, treating the cause. Use of orthotic therapy, for example, CMO, is an excellent initial regimen and a same-day solution for patients to achieve quick results fast, as it helps realign the body’s biomechanical structure and control any excessive foot pronation, eliminating the pull at the insertion point of the plantarfascial tear. But what if this doesn’t achieve the required results for the patient, then casted custom orthotics may be required. They also help stabilise the heel bone and the growth plate, reducing inflammation and pain. Gel and rubber gradient heel lifts are advertised to take the tension off the heels, but they do not address the cause of pain and can even create an unstable platform for everyday walking.
- Strapping: Exercises help to gently release any tension in the plantar fascia and reduce inflammation.
- Foot Mobilisation: To help re-align the bones of the foot to reduce the stress on the plantar fascia.
- Dry Needling: Creates an inflammatory response within the body to break down the scar tissue.
- Shockwave Therapy: Mechanical shocks stimulate a healing response to the affected plantar fascia.
- Injection Therapy: Including prolotherapy, cortisone, or neural therapy.
Orthotic Calibration and Footwear
Medically prescribed orthotics, for example, we will be using Crown Medical Orthotics as an example chart in understanding how to provide the appropriate orthotic type for the patient based on specific body weight and the total range of pronation (TROP):
Orthotic Type | Density | Kilogram | Trop |
|---|---|---|---|
Yellow | Soft | 45kg – 55kg | 0°- 5° |
Orange | Meduim | 55kg – 65kg | 5°- 10° |
Blue | Firm | 65kg – 100kg | 10°- 15° |
2/3 style 3 densities | 45kg - 65kg | 5°- 15° |
Taken from Crown Medical Orthotics (CMO) Chart
Over 15° Trop may require full customisation from a cast.
References & Further Reading
Primary Clinical Source
Najjarine, A.R. Clinical Biomechanics of the Lower Limbs using the NBA™ System. International Association of Clinical Biomechanics (IACB).
Clinical Resources
Dr Abbie Clinics. “Plantar Fasciitis: Assessment and Treatment.” drabbieclinics.com.au
About the Author
Dr A.R. NajjarineM.A.Pod.A, B App Sc Pod (QMU UK), Dip Hlth Pod (NSW), Dip REM Ther, Dip Sport Med, ACNT NSW, Cert Acup, Cert Mb/Adj SMA, AAPSM, IACB. Founder of the International Association of Clinical Biomechanics and lead clinician at Dr Abbie Clinics. Dr Najjarine is the developer of the NBA™ System for biomechanical correction of the lower limb.